
Information
Pre-diabetes is characterised by the presence of blood glucose levels that are higher than normal but not yet high enough to be classed as diabetes. If undiagnosed or untreated, pre-diabetes can develop into Type 2 Diabetes (T2D).
For this reason, pre-diabetes is often described as the grey area between normal blood sugar and diabetic levels and is a risk factor for cardiovascular disease and future Type 2 Diabetes.
Diagnosing Pre-diabetes
Pre-diabetes is a state of early insulin resistance and can be diagnosed with a single HbA1c of 42-47. It also encompasses impaired fasting glycaemia and impaired glucose tolerance.
If a pre-diabetes state is diagnosed using glucose criteria, HbA1c should be checked as a baseline and should be used for follow-up purposes. An individual with IFG and/or IGT may have an HbA1c ≤41 mmol/L at baseline, but they should still be diagnosed and coded as pre-diabetes.
| Situations where HbA1c may not be a reliable diagnostic test * | |
| Prolonged RBC survival (falsely ↑ HbA1c) | • Untreated IDA • Vit B12/folate deficiency • Post-splenectomy |
| Reduced red cell survival (falsely ↓ HbA1c) | • Haemolytic anaemia (e.g. G6PD def, hereditary spherocystosis) • Splenomegaly • Anti-retroviral drugs |
| Other | • Recent Blood Transfusion (falsely ↓ HbA1c) • Haemoglobinopathy (falsely ↓ or ↑ HbA1c) |
* As with diabetes diagnosis HbA1c is less reliable in these contexts. The HbA1c result should be interpreted with caution and if out of keeping with the clinical picture consider checking a fasting glucose and if the situation still unclear seeking advice from clinical biochemistry or specialist diabetes team. OGTT can also be used if doubt remains as with patients with gestational diabetes
Coding
In Lothian we recommend using the umbrella code Pre-diabetes (WITH the hyphen)*
#C11y5 Pre-diabetes
You may also wish to consider an additional recall code such as: 66Az High risk of diabetes annual review** However, consideration should be given to frailty when considering using this code. Practices may wish to assess frail patients on an individual basis to determine the appropriate frequency of monitoring.
* when performing future QI, audit or similar, we would still recommend you include R102.11 Pre-diabetes in searches for the condition to capture those coded this way historically.
** this code can be used for ALL high risk patients on one recall, includes Gestational diabetes, Long term high dose steroids (> 5mg for > 3 months), PCOS over 40Y)
These definitions are shown in Table 1 in the Resources and Links section. Note the recent change in fasting glucose threshold to align with updated SIGN guidelines 2025, fasting plasma glucose now 6.1-6.9.
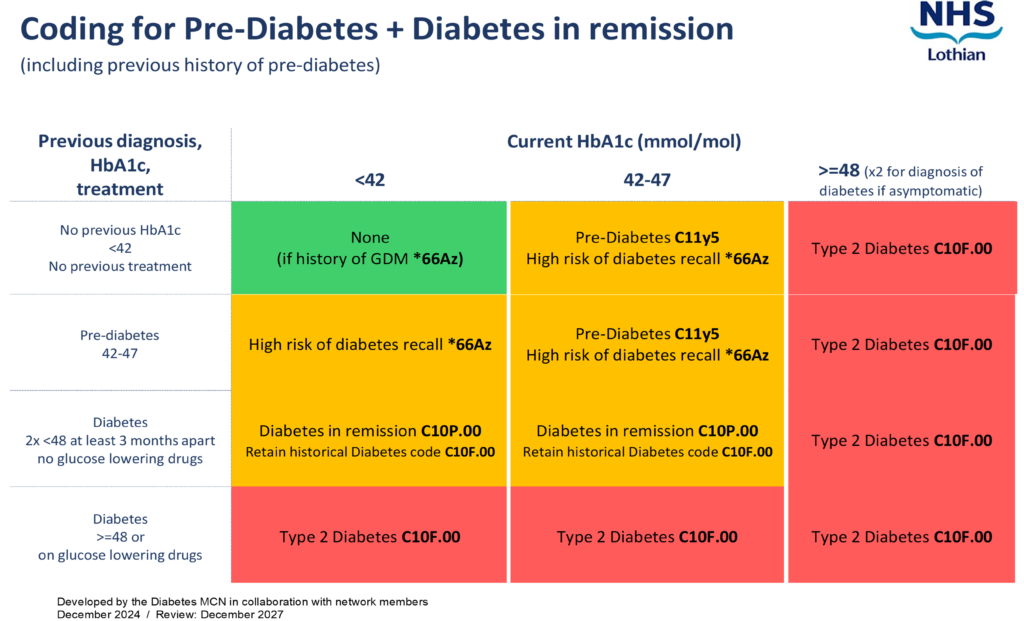
https://apps.nhslothian.scot/files/sites/2/Pre-diabetes-Dynamic-Coding-Infographic-December-2024.pdf
Let’s Prevent Diabetes Programme
LPD is a structured education programme for people with Pre-diabetes (HbA1c 42–47 mmol/mol), including Impaired Fasting Glycaemia (IFG) and others at high risk of Type 2 Diabetes.
Delivery Options:
- Face-to-Face: One 6-hour group session.
- Virtual: Three 2.5-hour sessions via Near Me.
- Self-Led Online: MyDESMOND web app for flexible learning; also available as a post-session resource.
Follow-Up: Review within 12 months, a 3-hour refresher session and updated self-management plan.
Referral Process: see referral guidelines section
M.A , S.S & A.C – 09-04-26
Who to refer:
Refer the following patients to the Let’s Prevent Diabetes Programme:
Pre-diabetes: Refer patients withPre-diabetes (HbA1C 42 – 47, impaired fasting glucose, impaired glucose tolerance), or patients who are at high risk of developing diabetes for other reasons (see primary care management tab for risk stratification). Please complete OGTT for those with sickle cell trait before referring.
PIL: Lets Prevent Diabetes.pdf
GDM: Patients that have had previous Gestational Diabetes (GDM) are at increased risk of future T2D, so those with GDM are automatically offered LPD post-partum as part of the Lothian GDM Pathway. But direct referrals to LPD / Prevent IT are welcomed at any time from this cohort.
PCOS: Patients with PCOS are often high risk. Consider risk stratification and testing.
Further information: NHS Lothian Adult Weight Management and Type 2 Diabetes Service web page
Who not to refer:
- Patients already diagnosed with T2D. Refer to DESMOND
- Patients with only a low/moderate risk of Diabetes (See details in Primary Care Management section)
- Patients who do not have a diagnosis of prediabetes but may require weight management support.
How to refer:
AHP – Dietetics – Let’s Prevent Diabetes – LI Let’s Prevent Diabetes
Referrals are accepted from all health care professionals via sci-gateway or by letter, email or referral form to Weight Management Mailbox.
Please visit Weight Management Service Adult – RefHelp (nhslothian.scot) page for more information.
Patients are able to self refer to Let’s Prevent Diabetes programme using this form Adult Weight management Referral form.pdf
Primary care teams play a significant role in the identification of patients with pre-diabetes, those who are at High risk of diabetes and also those at moderate risk of developing diabetes.
At risk groups include those known to be at increased risk of T2D, due to the risk factors below.
Risk Factors:
- Age: Over 40 years old (white Caucasian) or over 25 years old (African-Caribbean, Black African or South Asian)
- Family history: 2-6 times more likely to develop T2D if a parent, brother, sister or child has diabetes
- Ethnicity: T2D is 2-4 times more likely in people of South Asian descent and African-Caribbean or Black African descent*
- Overweight: BMI over 25 (white Caucasian) or over 23 (African Caribbean, Black African or South Asian)
- Waist circumference:
- Women: 31.5 (80-cm) inches or over
- Men: 35 (90 cm) inches in south Asian men, 37 (94cm) inches in white or black men
- High blood pressure or previous heart attack or stroke
- Polycystic ovary syndrome
- Previous gestational diabetes*
- Severe mental health problems including those prescribed Clozapine and Olanzapine which are known to induce weight gain and increase risk of T2D.
If a patient has a number of the above, the more at risk they are of developing T2D.
Encourage risk assessment for the following groups:
- all adults aged ≥40 (excluding pregnancy)
- individuals aged 25–39 from high-risk ethnic groups
- adults with conditions that increase the risk of type 2 diabetes (e.g. CVD, Huperension, obesity, strok, PCOS, gestational diabetes)
1. Calculate and code RISK score:
This can be calculated via the Diabetes UK Know Your Risk Tool, which requires patients to measure height, weight and waist circumference, or the Leicester diabetes score (abbreviated form the DUK know your risk tool) which is available on Vision+
NICE guidelines encourage keeping an up to date register of RISK scores, along with introducing a recall system to invite those at risk of Type 2 Diabetes in for regular review. This is also an opportunity to support patients to manage lifestyle changes and encourage goal setting.
2. Manage RISK score:
Please note SIGN guideline recommend FPG range 6.1-6.9 in line with WHO guidelines.
3. Lifestyle changes
Lifestyle changes with the aim of managing excess weight and increasing exercise are pivotal to the prevention of diabetes, but consider all the pillars of health
- Diet– There is no single ‘diet’ in diabetes, Aim for a healthy balanced dietary pattern with a move away from ultra processed, high carbohydrate containing foods towards more fibre rich wholegrains, fruit and vegetables, as able. There is some evidence for Mediterranean, DASH diet, whole foods, plant based and low carbohydrate diets but the most important changes are ones patients are motivated to stick with. For more information about the individual programmes for weight management visit Weight Management Service Adult – RefHelp (nhslothian.scot) .
- Physical Activity. National guidelines recommend trying to accrue minimum of 30 mins of Moderate Activity daily, or 210 mins over the week, when diagnosed with Prediabetes or Type 2 Diabetes. This is where the patient is breathing a little deeper and working a little harder than normal, although even little and often sustainable changes and breaking up sedentary time can start the process of improving outcomes.
- Physical Activity support can be offered & provided by Local partners via local pathways:
- Edinburgh Leisure Health and Wellbeing Support Programmes – Active Communities
- East Lothian Physical Activity Pathway https://apps.nhslothian.scot/refhelp/guidelines/rehabilitation/east-lothian-rehabilitation-service-elrs/east-lothian-exercise-pathway/
- West Lothian Physical Activity Pathway: physical Activity – West Lothian Council
- Midlothian Physical Activity Active Choices Pathway: Midlothian Active Choices (MAC) | Midlothian health activities | Midlothian Council
- Walking Scotland – New name for Paths for all : walking routes/ groups support: https://walkingscotland.org.uk/about-us/
4. Monitoring of Pre-diabetes
Pre-diabetes is monitored with an annual HbA1c**, unless symptoms develop prior to this. Those that have attended LPD, making changes and attempting to impact HbA1c levels should be offered a HbA1c test 3 months post LPD completion.
Advise patients to consult their GP if they develop the following symptoms:
- Polyuria
- Polydipsia
- Change in eyesight
- Weight loss
- Lethargy
- Thrush oral/genital
** HbA1c is not reliable for monitoring pre‑diabetes in certain conditions that prolong or reduce RBC survival e.g. anaemia, haemoglobinopathies, splenomegaly (see HbA1c & Haemoglobin variants – RefHelp); in these cases, use Oral Glucose Tolerance Test (OGTT).
Patient Friendly self-monitoring methods
Home monitoring of Blood pressure : https://www.nhsinform.scot/illnesses-and-conditions/cardiovascular-disease/risk-factors-for-cardiovascular-disease/high-blood-pressure-hypertension/
Waist Measurement https://www.diabetes.org.uk/about-diabetes/type-2-diabetes/waist-measurement
Monitoring Levels of Physical Activity through Activity diaries / charting /journaling
Monitoring Diet through food diary.
Smoking diary -possible setting of quit date https://www.nhsinform.scot/stopping-smoking/my-quit-plan
Drinking Diary Daily drinks diary – Your guide and record to success
| Normal | Pre-Diabetes | Diabetes | |
|---|---|---|---|
| HbA1c (mmol/mol) | ≤ 41 | 42-47 | ≥ 48 |
| Fasting glucose (mmol/l) | ≤ 5.4 | 6.1-6.9 | ≥ 7.0 |
| 2-hr glucose in OGTT (mmol/l) | ≤ 7.7 | 7.8-11.0 | ≥ 11.1 |
| Random glucose (mmol/l) | ≥ 11.1 |
Information for healthcare professionals
- Prevention and remission of T2DM SIGN Guidelines Prevention and remission of type 2 diabetes (SIGN) | Right Decisions (scot.nhs.uk)
At risk of T2D is defined as being at Moderate to High risk of T2D via the Diabetes UK Know Your Risk Tool
High risk T2D is defined as those with previous or current Gestational Diabetes, those with Poly Cystic Ovary Syndrome or those with Prediabetes.
Information for patients
- Pre-diabetes – Health Information
- MyWay ealearning: Type 2 Diabetes Prevention Online Course | Information Site (scot.nhs.uk)
- Diabetes UK: Prediabetes symptoms and risk reduction | Diabetes UK
- NHS Lothian Weight management service LPD: Lets Prevent Diabetes – Adult Weight Management and Type 2 Diabetes Prevention Service (nhslothian.scot)
- British Heart Foundation: Why your waist size matters – BHF
- Moving Medicine: physical activity information leaflets
- Primary_Prevention_Patient_info_leaflet_2020 (movingmedicine.ac.uk)
- Obesity2_Patient_info_leaflet_2022 (movingmedicine.ac.uk)
- Discuss harmful substance avoidance (alcohol/smoking)














