

Anaemia due to Iron deficiency
Please note that this guidance also applies to those with proven iron deficiency without anaemia, but please see below about the need for GI investigations.
Definition:
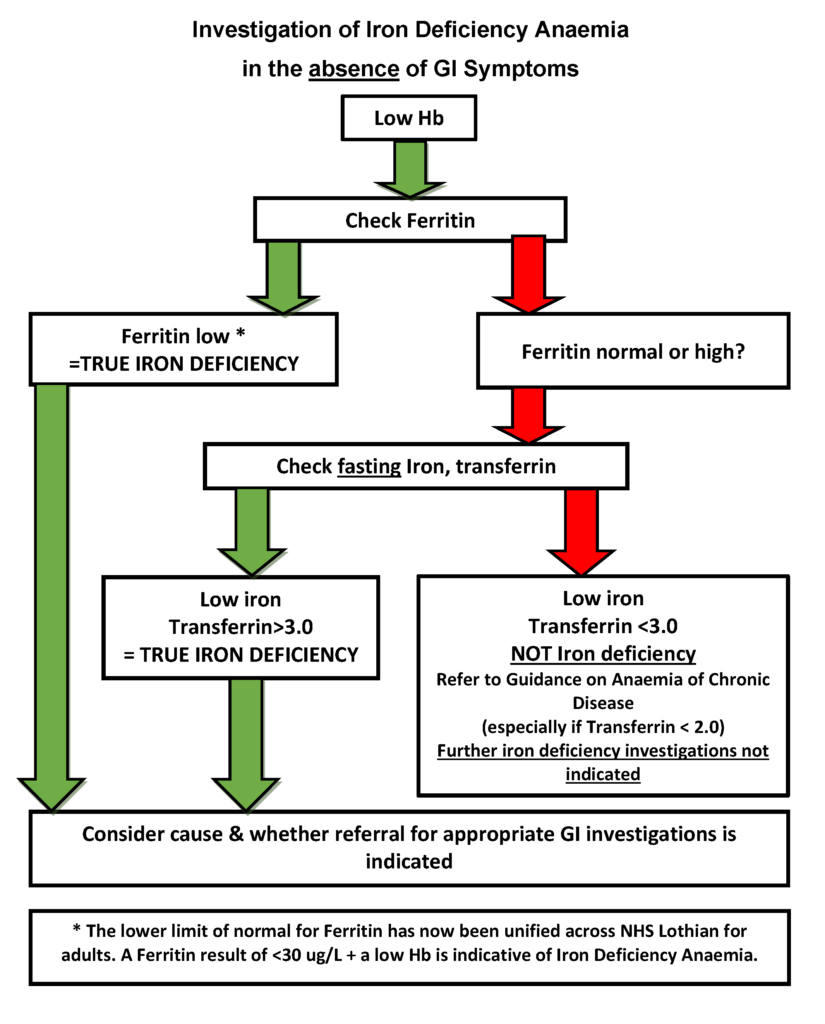
Anaemia (haemoglobin below normal range) and evidence of iron deficiency – this is defined by either:
- Low ferritin <30 ug/L* (Diagnostic of Iron deficiency)
- Normal ferritin in which case further iron studies are required on a fasting blood sample (take sample in morning with nothing to eat and only water to drink since midnight) – low serum iron and transferrin ≥3.0 g/l are then diagnostic of iron deficiency. Please see below for more detail.
*The Lower Limit of Normal for Ferritin has now been unified across NHS Lothian for Adults. A Ferritin result of <30 ug/L alongside a low Haemoglobin is indicative of Iron Deficiency Anaemia. This definition agrees with the guidance in the: Scottish Referral Guidelines for Suspected Cancer 2025
In all other cases of anaemia, please follow separate RefHelp guidance for those with microcytic, normocytic or macrocytic anaemia.
Iron deficiency without anaemia.
Endoscopic investigation rarely detects malignancy in patients with proven iron deficiency (low ferritin or normal ferritin with low serum iron and transferrin ≥3.0 g/l on a fasting blood sample), but without anaemia. GI investigations may be appropriate for patients >50 years (and without history of menorrhagia) with proven iron deficiency in the absence of anaemia.
Please note:
- Not all microcytic anaemias are caused by iron deficiency. It is essential to confirm iron deficiency to avoid unnecessary invasive investigations. Always perform a ferritin (low result is diagnostic of iron deficiency). However, since ferritin is an acute phase reactant, a normal or high ferritin does not exclude iron deficiency. In such cases, check serum iron and transferrin on a fasting blood sample; a low serum iron and transferrin ≥3.0 g/l are then diagnostic of iron deficiency.
- For microcytic anaemia not proved to be caused by iron deficiency, please see Inherited red cell disorders on RefHelp for appropriate management.
Treatment of Iron Deficiency.
Please see Iron Deficiency Treatment which also contains advice for when treatment is proving difficult, including the use of intravenous iron.
Updated C.M, A.K & J.B March 26
Who to refer:
- Patients with unexplained iron deficiency anaemia should be referred to GI as outlined in the Gastroenterology IDA RefHelp page
- As Menstruation is the most common cause of IDA in menstruating people under 50 years of age, then this group of patients can still be referred under the GI IDA Referral pathway, but they will be triaged to stool qFIT testing only and if double qFIT testing is negative they will not proceed to other GI investigations
- If under a parent specialty for bleeding symptoms, or with a clear organ system cause for iron deficiency, referral should be directed to the appropriate specialty.
- Iron deficiency anaemia where the patient is completely intolerant of all oral iron preparations and requires intravenous iron treatment – please refer to the involved specialist (and not haematology), who can arrange an infusion in the Medical Day Case Unit.
Who not to refer:
How to refer:
- Patients needing further investigation should be referred urgently to the Department of Gastroenterology WGH, St Johns or RIE as indicated above. Please see: Gastroenterology IDA RefHelp page
- Patients needing treatment with intravenous iron should be referred to specialist investigating their symptoms.
Primary care investigations
- Full history including menstrual history, GI history, medications, family history, dietary history
- Examination including abdominal exam looking for masses
- Ferritin
- If ferritin normal check iron and transferrin on a fasting blood sample
- If iron deficiency confirmed check coeliac screen
- Urinalysis for blood
British Society of Gastroenterology – Guidelines for the management of iron deficiency anaemia:














