
Cervical cancer affects all adult age groups, with above 50% of cases occurring between the ages of 30 and 50 years. 40% of new cervical cancer cases in women of screening age (25-64 years) were screen detected in Scotland in 2022.
All patients with abnormal bleeding (IMB / PCB / PMB) or excessive discharge (+/- pelvic pain) should have a speculum examination to rule out a cervical / vaginal / vulval malignancy.
A smear is not required unless indicated by SCCRS guidance e.g. smear due or previously defaulted. Cervical sampling is intended to be used as a screening tool to detect pre-cancerous changes in asymptomatic people, not for diagnosing symptomatic cancers. Most cervical lesions are benign and may be referred routinely to general gynaecology
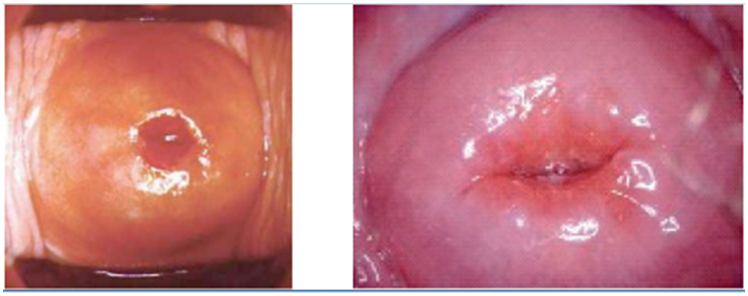
Normal cervix
Atrophic cervix / vagina
Cervix +/- vagina may appear vascular / red after menopause due to atrophy
→ May benefit from topical estrogen if symptomatic
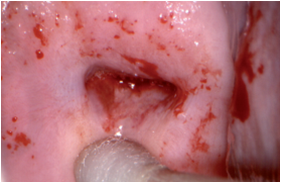
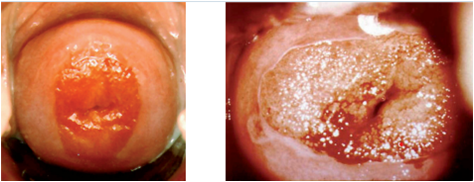
Cervical Cancer
Fungating +/- ulcerated lesions, irregular, friable
→ Refer to colposcopy as USOC
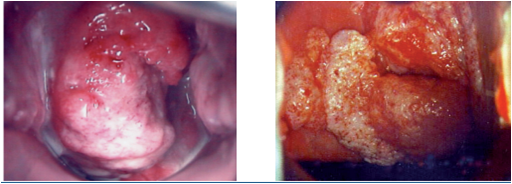
Cervical polyps
Usually benign / smooth outpouching of the lining of the cervix
→ Refer routinely to general gynaecology for removal
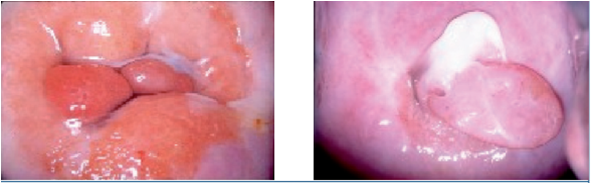
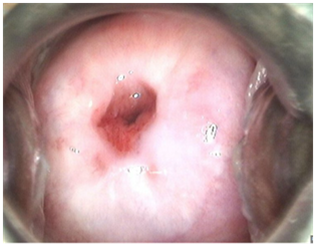
Cervical ectropion / ectopy Physiological
→ Only requires treatment if causing bothersome symptoms (PCB or excessive discharge) and patient wishes intervention
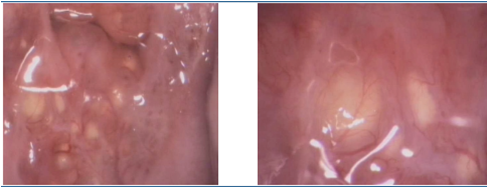
Nabothian follicles Physiological (blocked glands)
→ No intervention required
Prior LETZ treatment (at colposcopy)
Scarring / may appear like an ectropion / will persist after menopause
→ Manage like an ectropion
All the images above are with permission from the NHS Cancer Screening Programmes.
B.C. & L.P. 29-1-26
Colposcopy (USOC)
- Abnormal smears – these patients will be referred via SCCRS
- Suspicion of cervical malignancy on speculum examination
Sci Gateway>RIE/SJH>Gynaecology – Colposcopy (choose URGENT REFERRAL in protocol text and priority USOC)
General Gynaecology (USOC)
- Suspicion of vulval or vaginal malignancy
Sci Gateway>RIE/SJH>Gynaecology>LI Gynae Basic Sign Referral (priority USOC)
General Gynaecology (routine)
- Cervical Polyps
- Cervical ectropion – ONLY if causing bothersome symptoms and patient wishes intervention
Sci Gateway>RIE/SJH>Gynaecology>LI Gynae Basic Sign Referral (priority routine)
Please see also Scottish Referral Guidelines for Suspected Cancer 2025
Cervical screening | National Services Scotland
Scottish Cervical Screening Programme: https://www.nsd.scot.nhs.uk/services/screening/cervicalscreening/
changes-to-cervical-screening-programme-faq.pdf
cervical-screening-routine-pathway-diagram-march-2022.pdf
Useful Patient information
NHS Inform
Colposcopy https://www.nhsinform.scot/tests-and-treatments/non-surgical-procedures/colposcopy
Cervical Screening/Smear test https://www.nhsinform.scot/healthy-living/screening/cervical/cervical-screening-smear-test
The eve appeal We are the leading gynaecological cancers charity – The Eve Appeal














