

Please see Psychogenic versus organic Erectile Dysfunction
Please see Erectile Dysfunction Severe Distress Assessment in the Updated Sexual Health – Erectile Dysfunction Page
R.M & H.S 13-05-20
Who to refer:
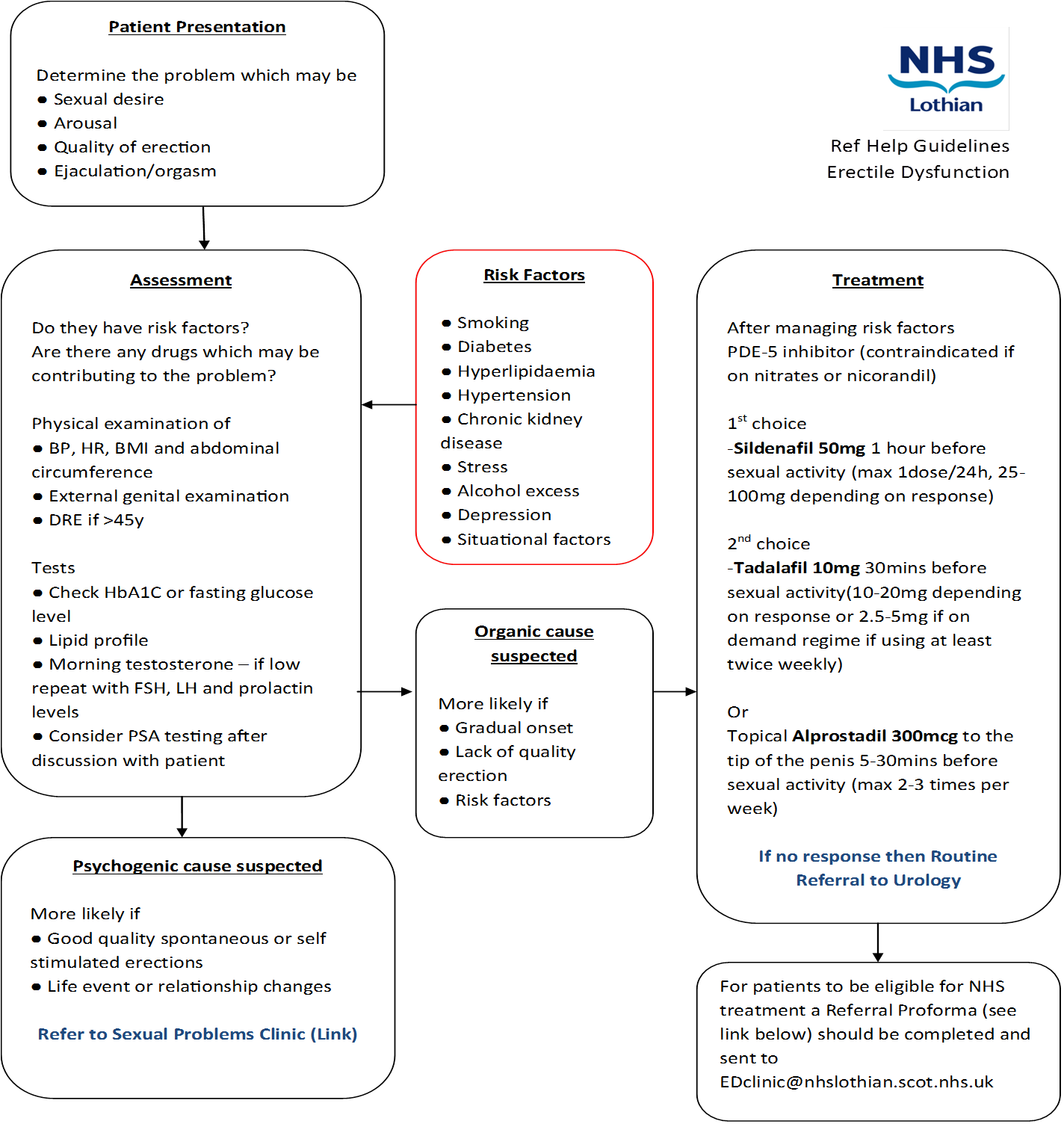
- If psychogenic cause of ED suspected – Refer to Sexual Problems Clinic
- If no response to oral or topical treatment – Refer as routine
Who not to refer:
- Patients who’s risk factors and/or drugs contributing to the problem have not been addressed
- Patients who respond to treatment
How to refer:
Through SCI gateway Western General Hospital Urology
Treatment – Erectile Dysfunction
Patients can and should be informed that there is a range of treatments which will help to resolve their problem. Almost all patients can be treated, provided they are prepared to use second line (intracavernosal self injection, vacuum pump, MUSE) and third line (penile implant) treatment options. They should be encouraged to report back if first line treatment (tablets) fail. While we recommend that only first line treatment is carried out in Routine General Practice, there is further explanation of other treatment options listed for information and as a reference for discussion with patients.
5 – Phosphodiesterase Inhibitors
This is the first line treatment for most patients. There is no direct comparison between the three 5-PDE inhibitors in good quality comparative trials, but essentially they all work similarly well in terms of efficacy, safety and tolerability. The overall efficacy in the broad population is around 68%, with a lower response rate in difficult patients such as diabetics (48%-56%).
Contraindication to all 5-PDE inhibitors are short or long acting nitrates. However it may be worth considering whether patients really need their nitrates. For instance some patients may have a GTN spray for angina, which they rarely use. These might be suitable for discontinuing their nitrates.
—FOR DISCUSSION: (or possibly start a shorter acting 5 PDE inhibitor under specific instructions that they absolutely must avoid taking/being given nitrates while have taken the 5 PDE inhibitor – this requires good patient compliance!).—
Others may be considered for change of long acting nitrates to other drug groups at their next cardiology review.
Dosage:
There is a “learning curve” for these drugs.
1. We recommend a course of 8 tablets for initial trial.
2. Most patients with complete erectile failure should be commenced on the higher treatment doses to benefit from the reassurance gained by successful treatment initially (they can try to reduce the dosage later). Only patients with neurological disease and those with partial ED should be started on the lower doses.
3. Patients need to be advised that these drugs only work with concomitant adequate sexual stimulation.
4. Patients need to be informed about the optimum time for intercourse in relation to drug intake.
| Max. levels | Half life | Cost in £ | ++ PRO ++ | — CON — | |
| Sildenafil (Viagra) max. once daily | 70 min | 3.8 hrs | 100 mg 8-tab = 46.99 (4-tab = 23.50) 50 mg 8-tab = 38.67 25 mg 8-tab = 33.19 | Best evaluated safety profile | Avoid: retinitis pigmentosa |
| Vardenafil (Levitra) max. once daily | 40 min | 3.9 hrs | 20 mg 8-tab = 46.99 (4-tab = 23.50) 10 mg 8-tab = 38.67 5 mg 8-tab = 33.19 | Early onset – spontaneity | |
| Tadalafil (Cialis) max. once daily | 120 min | 17.5 hrs | 20 mg 8-tab = 46.79 (4-tab = 23.40) 10 mg 4-tab = 23.40 | Long acting | Risk of back pain & myalgia |
5. Drugs may be effective before reaching maximum levels, 30 minutes is a reasonably good time point for sildenafil and vardenafil. Some vardenafil patients report even more rapid onset after as little as 15 minutes, possibly allowing for more spontaneity. The window of efficacy for sildenafil and vardenafil is around 8 hours, but tadalafil may still work for up to 36 hrs, possibly allowing intercourse at a later time point.
6. Normal meals delay the absorption of sildenafil, fatty meals delay absorption of sildenafil and vardenafil and patients need to know this. Tadalafil absorption is probably not significantly affected by fatty meals.
Safety & Side effects of 5-Phosphodiesterase inhibitors:
All 5 PDE inhibitors have similar transient side effects of: headache, flushing, indigestion and a stuffy nose. The frequency of side effects is dose dependant and duration similar for all drugs. Vomiting, dizziness, painful red eyes and raised intra-ocular pressure may also occur. Hypersensitivity reactions and priapism (see below) are rare.
Sildenafil has a low incidence of visual side effects, typically blue colour changes and a bright vision (only rarely seen with vardenafil and not with tadalafil). There are no permanent visual effects, but sildenafil is contraindicated in retinitis pigmentosa.
Tadalafil alone has possible side effects of back pain and myalgia.
Cardiac safety: There is no increased incidence of myocardial infarction with these drugs. All drugs are contraindicated in patients taking nitrates as they potentiate their effect. 5 PDE inhibitors also interfere with alpha-blockers. (This may be circumvented in patients taking alpha-blockers for bladder outflow obstruction by taking the alpha-blocker in the morning and the 5PDE inhibitor in the evening, eg. Tamsulozin. Alfusozin, Prazosin, Terazosin.)
Patients with significant cardiac disease should be assessed cardiologically before using 5PDE inhibitors (see below).
Sexual activity is mild exercise and should be within the physical capacity of most men. Peak heart rates and systolic pressures achieved during intercourse only reach 60-70% of the maximum values achieved in a treadmill test. The workload equates with walking at 3 miles per hour on the flat for older men or with walking at 4.2 mile per hour up a 16% gradient (or cycling at 10 miles per hour) for younger men.
Priapism: this very rare, but potentially devastating complication of a prolonged painful erection of more than 4 hours is an emergency requiring immediate treatment. Patients should be warned about it, so they can seek help early. Latest after 24 hrs smooth muscle necrosis occurs, resulting in impotence. Click here for treatment advice!
NHS PRESCRIPTION SCHEDULE
Drugs for treatment of erectile dysfunction may only be prescribed on the NHS under certain circumstances.
Treatment is licensed for patients with:
1. diabetes mellitus
2. multiple sclerosis, Parkinson’s disease, poliomyelitis,
3. single gene neurological disease, spina bifida, spinal cord injury,
4. kidney transplant or on dialysis for renal failure,
5. prostate cancer,
6. severe pelvic injury, radical pelvic surgery, prostatectomy
7. or were receiving treatment for ED at NHS cost on 14th September 1998.
The Department of Health (England) has recommended that treatment should also be available from specialist services when the condition is causing severe distress.
Criteria for distress are:
1. significant disruption to normal social and occupational activities,
2. a marked effect on mood, behaviour, social and environmental awareness,
3. or a marked effect on interpersonal relationships.
Severe distress category prescriptions are meant to be issued in Specialist Hospital clinics. However apart from the fact that the higher surgical curriculum does not include psychological or psychiatric training to assess such patients it is also reality that NHS Lothian does not provide any funds to specialist services for such hospital prescriptions at present. As such prescriptions cannot be issued through secondary care at present. This issue has been repeatedly raised with management team in Urology. The recent development of a general practitioner being penalized for prescribing 5PDEI’s to a patient in severe distress without consulting secondary care first has brought this issue in focus. It is now being taken forward to the Trust Board for a solution. At present referrals for severe distress assessment in the Urology clinics have been put on hold until the prescription issue has been addressed.
It may be of note that the term prostatectomy includes TURP.
Secondary care can offer further assessment and initial free testing of second line treatments in the clinic, but other treatment costs for secondary care treatments will have to be addressed as above.














