
Sudden sensorineural hearing loss is an otological emergency – please contact ENT on call same day – see Referral Guidelines below for further detail, including of the ‘Starfish’ trial
Presentation of Sudden Sensorineural Hearing Loss (SSNHL)
- A rapid loss of hearing that occurs suddenly or over a period of up to 72 hours
- Typically unilateral
- Mean age of presentation 30-60 years
- Estimated incidence in adults of between 5 and 30 cases per 100,000/year
- Sometimes associated with tinnitus/vertigo.
Causes
- Idiopathic – commonest cause
- Infection – viral (e.g. mumps, cytomegalovirus, varicella/zoster), bacterial (syphilis, meningitis)
- Autoimmune – Sarcoidosis, Wegener granulomatosis
- Vascular – Hypercoagulable states
- Tumour – Vestibular Schwannoma, temporal bone metastases
- Trauma – Temporal bone fracture, acoustic trauma, head injury
- Drugs – Aminoglycoside antimicrobials, cisplatin.
Prognosis
Spontaneous recovery from SSNHL varies in studies from 47-63% with the caveat that different studies used different criteria for degrees of recovery. Period of recovery varies from days to weeks. Poor prognostic indicators include:
- Age: <15 and >65 years
- Associated vertigo/imbalance
- High frequency/profound hearing loss
- Bilateral hearing loss.
STARFISH TRIAL.
ENT is conducting a randomised controlled trial to assess best treatment and it is crucial that patients have not received prior steroids. The ‘Starfish’ RCT will examine the outcomes relating to route of steroid administration – oral vs intratympanic vs both:
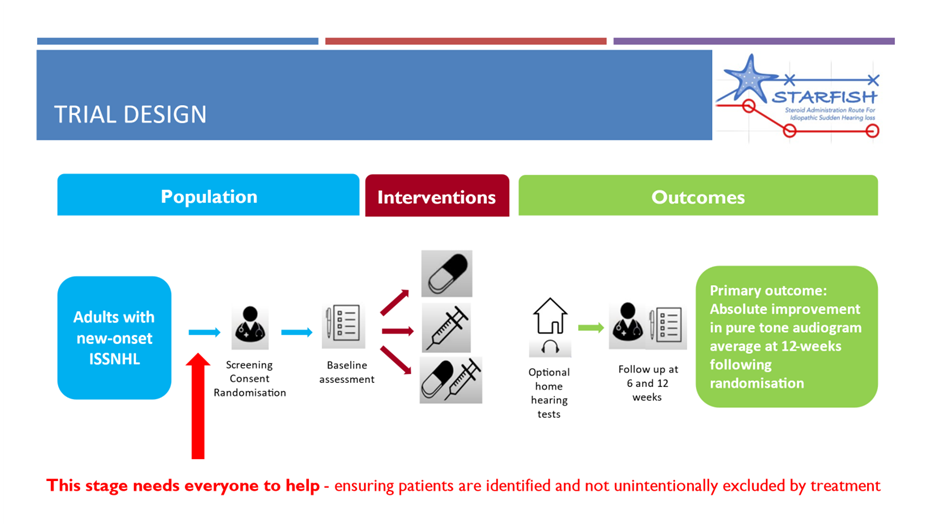
Those not wishing to participate in the trial will be offered high dose oral steroids (current standard practice)- but please note that the majority of those currently referred for this indication do not require them as they have normal audiograms or another explanation for their hearing loss.
For further details please see the STARFISH trial website.
C.M. & A.B. 02-12-24
Who to refer:
Any patient presenting within one week of onset of sudden sensorineural hearing loss. This is an otological emergency.
Who not to refer:
Patients with no evidence of sensorineural hearing loss on examination, or who clearly have another cause for hearing loss.
How to refer:
Please refer the same day by contacting the ENT on Call via St John’s Hospital, Livingston via switchboard.
Please do not prescribe oral steroids prior to assessment by ENT – the majority referred do not have sensorineural loss when further assessed and steroids contribute to iatrogenic harm. It is helpful to mention the Starfish trial to patients at the point of referral so that they are aware of what they might be offered when seen.
The on-call ENT clinician will ask on the telephone call for all the following, and patients do need to be physically examined by the referring clinician:
- Failed whisper test – this is crucial to reliably establish hearing loss
- Positive or false negative Rinne tuning fork test – wherever possible – to help distinguish conductive vs neurological hearing loss
- No other explanation for fluctuation in hearing from clinical history, examination or the medical record
- No glue ear / wax <90% occlusion of canal.
Management by ENT
- Relevant history taking to establish a cause
- Otoscopic/microscopic examination of the ear
- Audiometric assessment
- MRI/CT – inner ear/brain – to exclude a retrocochlear cause like acoustic neuroma
- Targeted blood studies based on history to ascertain a systemic causes
- Follow up audiometry and referral for hearing aid if needed
- Decision about treatment including modality with offer of the Starfish RCT
Discuss any case over the phone (contacting the ENT on Call via St John’s, Livingston).














