

MSK Physiotherapy for people with cervical spine problems is provided as part of the NHS Lothian Integrated Spinal Pathway.
The NHS Lothian integrated spinal pathway is a multidisciplinary collaboration. The service is based on the principles of the right care, from the right person, at the right time in the right place. The service offers a single point of access for patients with routine spinal pain, lumbar spine related leg symptoms/ cervical spine related arm symptoms who require referral for their problem following failure to improve with initial primary care management.
Once within the service patients will be able to access all the multidisciplinary services that are required for their problem including physiotherapy, investigation, surgical opinion and pain clinic opinion. There will be no need for patients to return to their GP to seek additional referrals or investigations for the lumbar spine problem. The service is underpinned by agreed pathways, escalation criteria and multidisciplinary clinics.
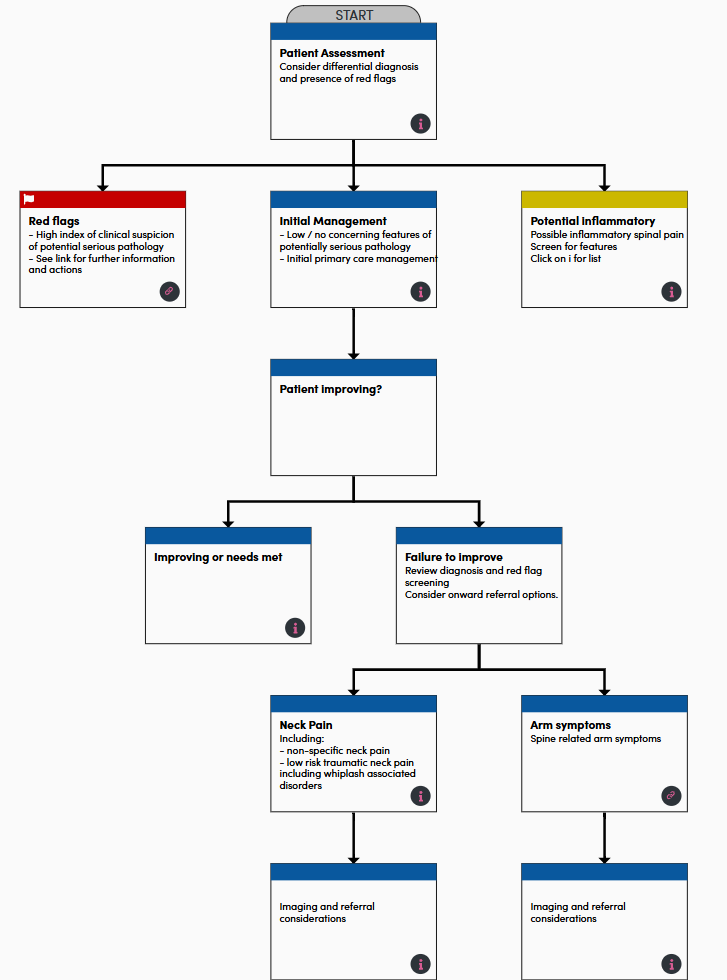
The information is also available on Primary care clinician within NHS Lothian – Cervical spine pathway | Right Decisions with interactive version of the flowchart above.
For patients & professionals – Integrated Spinal Service – NHS Lothian | Our Services
M.A & P.A. 14-05-26
Who can refer
- All primary care clinicians i.e. GPs, Primary care MSK advanced practice physiotherapists, advanced nurse practitioners
- Patient self referral (resident of East Lothian HSCP, Edinburgh HSCP and West Lothian HSCP Where To Find Us – Musculoskeletal Physiotherapy)
- Secondary care consultants and associated teams
- MSK physiotherapists are able to escalate/refer to advanced practice physiotherapists underpinned by agreed pathways and processes MSK physiotherapy within NHS Lothian (services included in pilot only) – Cervical spine pathway | Right Decisions
Who to refer:
- All routine cases of cervical spine pain and cervical spine related arm symptoms who have not responded to initial primary care management within a 4-6 week period and do not have the presence of significant red flags nor have suspected inflammatory spinal pain – see sections serious cervical spine conditions and other considerations and inflammatory spinal pain
- Cervical Spine related arm symptoms- Consider earlier referral in cases intractable symptoms and/ or developing motor deficit but without significant red flags
- Non-specific cervical spine pain in the absence of a dominant psychological component who have not received recent physiotherapy for their condition or who have received physiotherapy previously for their condition but;
- have experienced a substantial change in their presentation
- require assistance with achieving a functional goal
- wish further assessment and considerations of management options
- have clinical features suggestive of an underlying specific cause for their cervical spine pain, in which further investigation would guide management (other than serious spinal pathology).
- Non-specific cervical spine pain in the absence of a dominant psychological component who have not received recent physiotherapy for their condition or who have received physiotherapy previously for their condition but;
- For further support & guidance and refer to: Spine pathways | Right Decisions (scot.nhs.uk)
- Additional information regarding imaging available for xray and MRI found at radiology ref help spine Plain X-Rays – RefHelp
Who not to refer
- Patients who have the presence of significant red flags/ suspicion of serious cervical spine condition or have suspected inflammatory spinal pain – see Serious cervical spine conditions (Red Flags) – RefHelp
- Age <16
- Chronic cervical spine pain with a significant psychological / psychiatric / drug addiction element/ pain causing significant distress & disability, no planned referral to another speciality for diagnosis or treatment of pain – see Chronic pain Chronic Pain – RefHelp.
How to refer
- For all cases of routine cervical spine pain / spine related arm symptoms– refer via SCI Gateway Referral “AHP-Physiotherapy” then choose local site.
- This single referral will gain access to the full multidisciplinary NHS Lothian integrated back pain pathway. Any subsequent investigation/ surgical opinion/ pain service referral will be made within the service
- Please include all relevant details on your referral to allow the appropriate initial triage of the patient. Initial triage will occur within MSK Physiotherapy and if appropriate will be passed to spinal advanced practice physiotherapy service.
- Please signpost patients to Integrated Spinal Service Webpage for patient information.
Other information
For all routine cases of cervical spine pain and cervical spine related arm symptoms who meet the criteria under “who to refer”, referral to other specialities including Orthopaedics, Neurosurgery, Neurology & Rheumatology is not indicated. Once within the service patients will be able to access all the multidisciplinary services that are required for their problem including physiotherapy, investigation, surgical opinion and pain clinic opinion. There will be no need for patients to return to their GP to seek additional referrals or investigations for the cervical spine problem. The service is underpinned by agreed pathways, escalation criteria and multidisciplinary clinics.
For further information see associated sections
- Link to NHS Lothian patient internet site including patient information resources – Neck Pain – Musculoskeletal Physiotherapy
- Link to NHS Inform page cervical spine problems –Neck problems | NHS inform
- Link to NHS Inform page- neck conditions Neck and back problems and conditions | NHS inform
- Link to NHS Inform page- Exercises for neck problems Exercises for neck muscle and joint problems | NHS inform
- Link to intranet site NHS Lothian Integrated Spinal Service Integrated Spinal Service – NHS Lothian | Our Services














